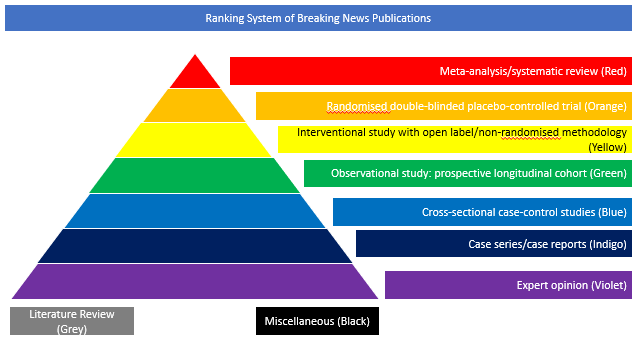
Randomised double-blinded placebo-controlled trial (Orange)
In this study recently published in The New England Journal of Medicine, the authors performed a randomised, double-blind, placebo-controlled trial involving patients with confirmed SARS-CoV-2 infection, hyperinflammatory states, and at least two of the following signs: fever (body temperature >38°C), pulmonary infiltrates, or the need for supplemental oxygen in order to maintain an oxygen saturation greater than 92%. Patients were randomly assigned in a 2:1 ratio to receive standard care plus a single dose of either tocilizumab (8 mg per kilogram of body weight) or placebo. The primary outcome was intubation or death, assessed in a time-to-event analysis. The secondary efficacy outcomes were clinical worsening and discontinuation of supplemental oxygen among patients who had been receiving it at baseline, both assessed in time-to-event analyses. 243 patients were enrolled; 141 (58%) were men, and 102 (42%) were women.
The median age was 59.8 years (range, 21.7 to 85.4). The hazard ratio for intubation or death in the tocilizumab group as compared with the placebo group was 0.83 (95% confidence interval [CI], 0.38 to 1.81; P=0.64), and the hazard ratio for disease worsening was 1.11 (95% CI, 0.59 to 2.10; P=0.73). At 14 days, 18.0% of the patients in the tocilizumab group and 14.9% of the patients in the placebo group had had worsening of disease. The median time to discontinuation of supplemental oxygen was 5.0 days (95% CI, 3.8 to 7.6) in the tocilizumab group and 4.9 days (95% CI, 3.8 to 7.8) in the placebo group (P=0.69). At 14 days, 24.6% of the patients in the tocilizumab group and 21.2% of the patients in the placebo group were still receiving supplemental oxygen. Patients who received tocilizumab had fewer serious infections than patients who received placebo. The authors concluded that tocilizumab was not effective for preventing intubation or death in moderately ill hospitalised patients with Covid-19. Some benefit or harm cannot be ruled out, however, because the confidence intervals for efficacy comparisons were wide.