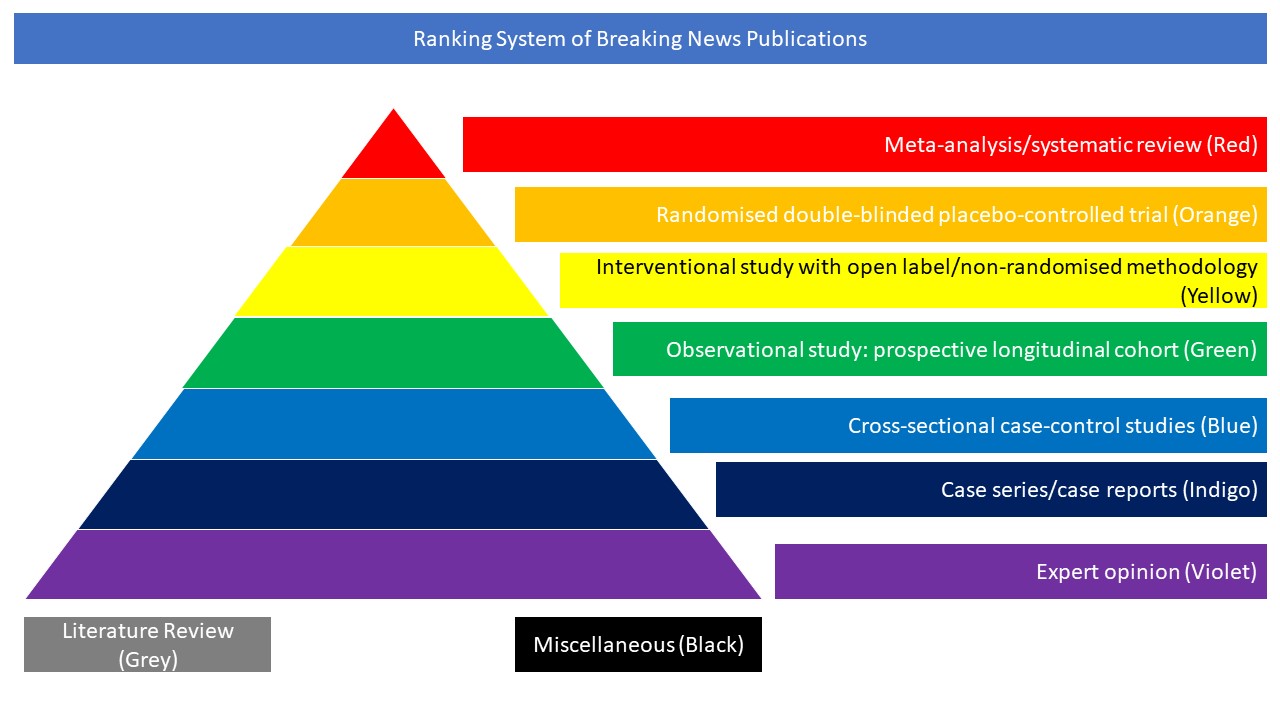
Cross-sectional case-control studies (Blue)
The objective of this observational cohort study was to evaluate whether early initiation of prophylactic anticoagulation compared with no anticoagulation was associated with decreased risk of death among patients admitted to hospital with COVID-19 in the United States. All 4297 patients admitted to hospital from 1 March to 31 July 2020 with laboratory confirmed SARS-CoV-2 infection and without a history of anticoagulation were enrolled. The main outcome was 30 day mortality. Secondary outcomes were inpatient mortality, initiating therapeutic anticoagulation (a proxy for clinical deterioration, including thromboembolic events), and bleeding that required transfusion. Of 4297 patients admitted to hospital with COVID-19, 3627 (84.4%) received prophylactic anticoagulation within 24 hours of admission. More than 99% (n=3600) of treated patients received subcutaneous heparin or enoxaparin. 622 deaths occurred within 30 days of hospital admission, 513 among those who received prophylactic anticoagulation. Most deaths (510/622, 82%) occurred during hospital stay. Using inverse probability of treatment weighted analyses, the cumulative incidence of mortality at 30 days was 14.3% (95% confidence interval 13.1% to 15.5%) among those who received prophylactic anticoagulation and 18.7% (15.1% to 22.9%) among those who did not. Compared with patients who did not receive prophylactic anticoagulation, those who did had a 27% decreased risk for 30 day mortality (hazard ratio 0.73, 95% confidence interval 0.66 to 0.81). Similar associations were found for inpatient mortality and initiation of therapeutic anticoagulation. Receipt of prophylactic anticoagulation was not associated with increased risk of bleeding that required transfusion (hazard ratio 0.87, 0.71 to 1.05). Quantitative bias analysis showed that results were robust to unmeasured confounding (e-value lower 95% confidence interval 1.77 for 30 day mortality). Results persisted in several sensitivity analyses. The authors concluded that early initiation of prophylactic anticoagulation compared with no anticoagulation among patients admitted to hospital with COVID-19 was associated with a decreased risk of 30 day mortality and no increased risk of serious bleeding events. These findings provide strong real world evidence to support guidelines recommending the use of prophylactic anticoagulation as initial treatment for patients with COVID-19 on hospital admission.
DOI: https://doi.org/10.1136/bmj.n311